Absolute vs Relative Risk
An exceptionally important medical statistic
In my last commentary, one of several key things I am recommending that RFKjr fix in the FDA, is how they portray effectiveness (of drugs, vaccines, etc.) to the public. Currently, the effectiveness that is almost exclusively shown is relative risk. I am advocating that absolute risk be shown. I cited two important examples where others have (so far unsuccessfully) made a case for the same thing:
Example 1: This position is stated in an important FDA advisory publication. A key conclusion (see page 60) is that the public is: “unduly influenced when risk information is presented using a relative risk approach; this can result in suboptimal decisions. Thus, an absolute risk format should be used.”
Example 2: The CONSORT 2010 Statement —Updated Guidelines for Reporting Parallel Group Randomized Trials states: “… presentation of both absolute and relative effect sizes is recommended…”
Since statistics is over most people’s heads, several readers asked me to explain the difference. OK, here goes…
I’ll use COVID-19 vaccines as a telling example. I put together three tables (below) based on two studies: here and here. (If you’d like further elaboration, here is an MD’s good discussion about those two studies.)
The first table shows the relative effectiveness of several popular COVID-19 vaccines:
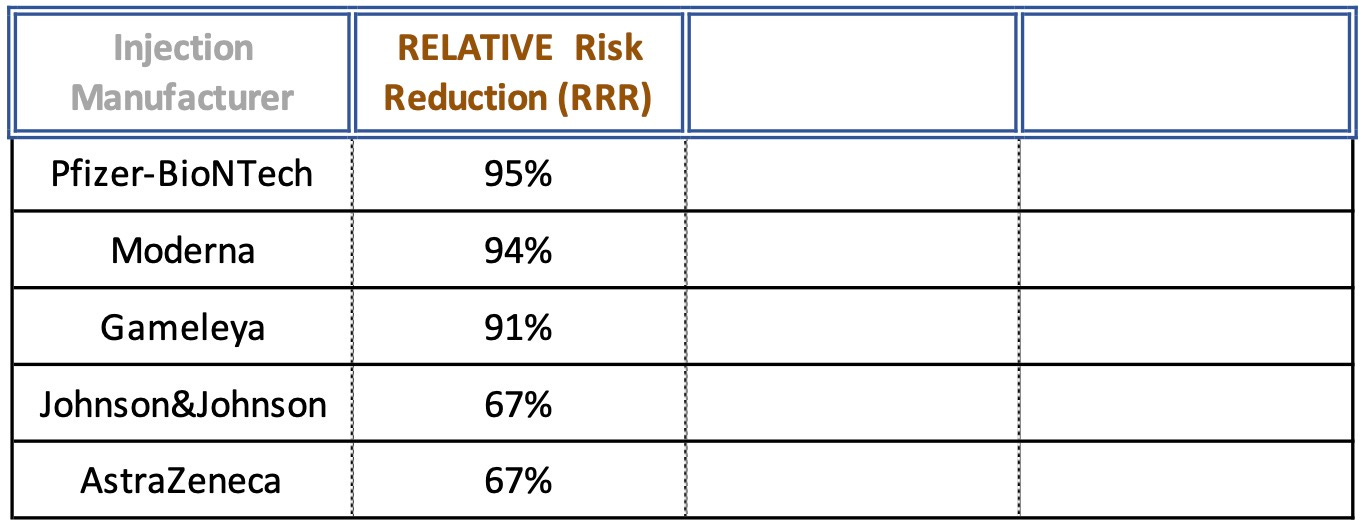
Now most people would say that these are good numbers — and the ones above 90% are VERY good. That’s exactly what the FDA and the pharmaceutical companies want us to think… Now let’s fill out the next column: absolute risk…
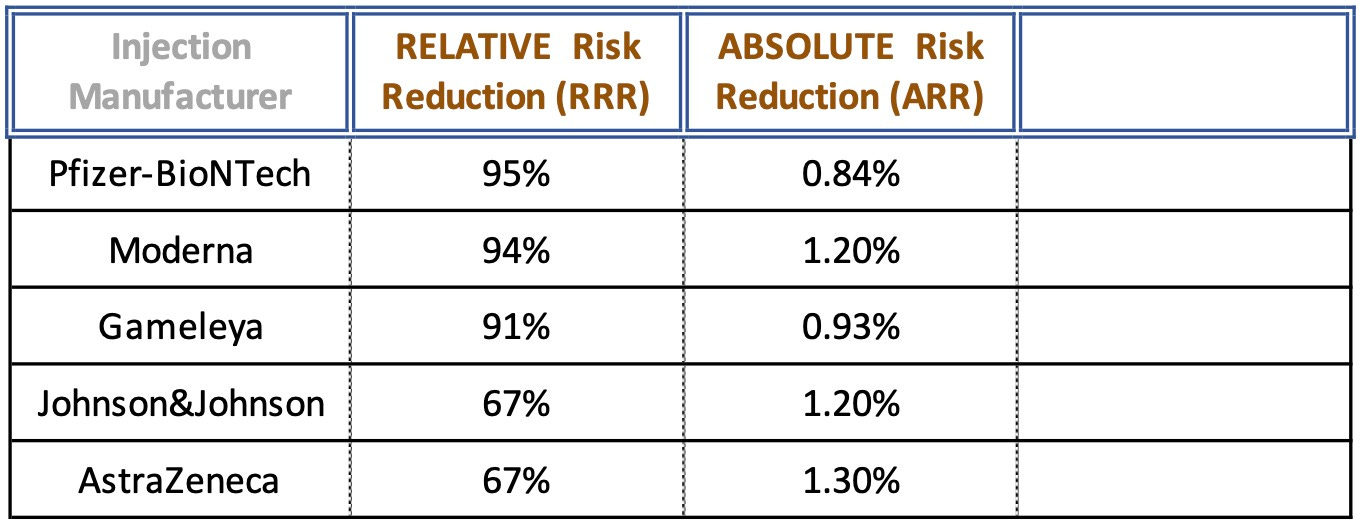
Whoa! The absolute numbers are radically different — and MUCH less! What does this mean in the real world? A third variable might be the easiest to understand: how many people need to be treated (injected) to prevent ONE case of COVID-19?
This is called NNT (Number Needed to Treat = 1/ARR). Here is a study that delves into the merit of using NNT. The table below shows what NNT is for the same COVID-19 injections:
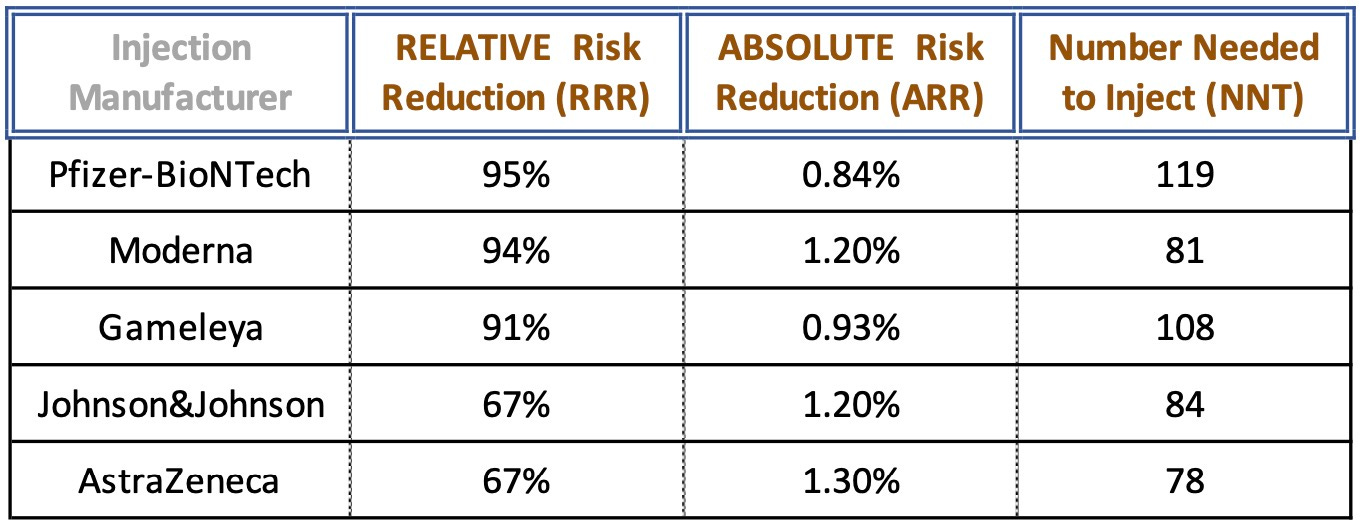
NOTE: The exact numbers here may be slightly different due to several variables, and are not important. What is significant is to see the extraordinary differences between Relative and Absolute Risk Reductions.
NNT Observation —
Let’s look at a real-world example… If citizens realized that roughly one hundred people had to be injected before ONE case of COVID-19 was prevented, would very many people have said:
“I’m willing to risk the known potentially serious side-effects of these injections, plus accept the fact that zero long-term studies have been completed, in the hopes that I’ll hit the jackpot and be the lucky one in 100± people who is prevented from getting COVID-19”?
The answer to that is why the FDA (and pharmaceutical companies) emphasize the Relative effectiveness number.
An Even Better Analysis —
Some very smart people said let’s take the NNT data one step further — and add the treatment cost to it! In other words, if two treatments have the same NNT, but one costs 10 times the other, shouldn’t we factor that in? Look at this fabulous COVID-19 table:
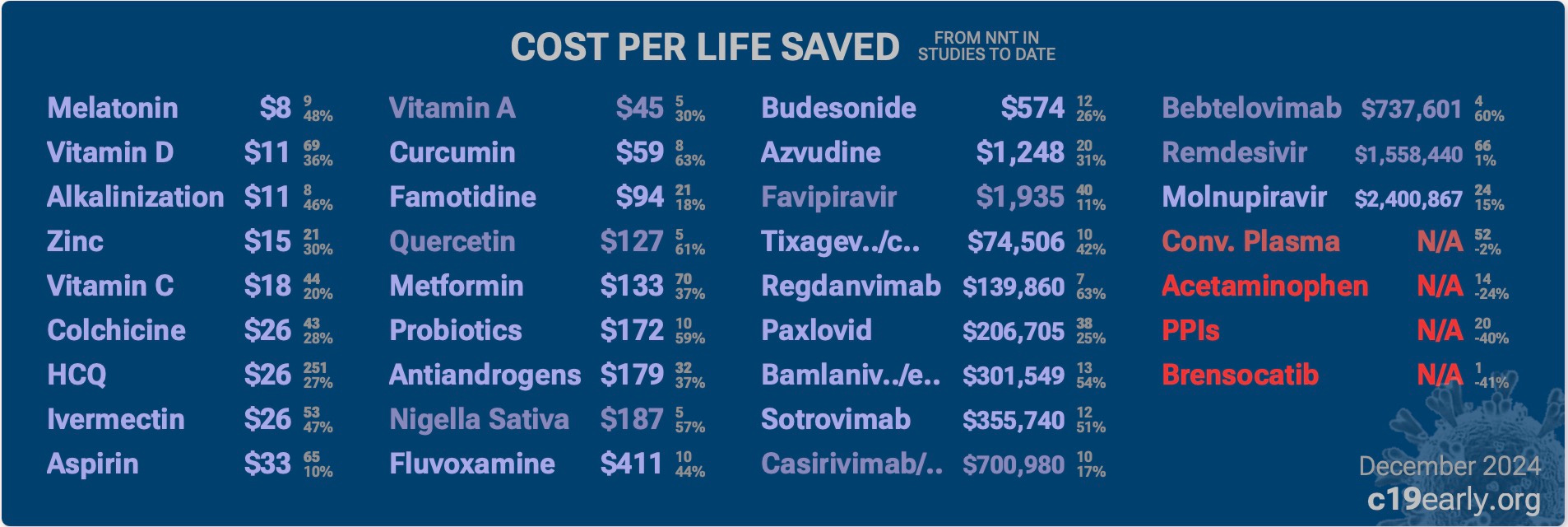
Compare two COVID-19 early oral treatment competitors: Ivermectin and Paxlovid. To get the same end result (save one life from COVID-19) we can spend $26 for Ivermectin or $206,705 for Paxlovid… Note also that cost and impacts of side-effects are not taken into account here. The side-effects for taking Ivermectin are very low, while the potential side-effects for Paxlovid are relatively high. In other words, the cost difference between Ivermectin and Paxlovid is likely MUCH more that what is shown in this table!
Takeaway —
My recommendation to RFKjr is that (as a minimum) BOTH Relative and Absolute numbers should be prominently displayed, as well as NNT. This is not some academic matter, as it has GREAT bearing on assuring that Americans are able to make an informed consent when they agree to an injection or to take a drug. Without the facts, we are severely handicapped in being a critical thinker.
PS — Here is an excellent two minute video that explains the difference between Absolute and Relative Risk reduction…
PPS — Just like here, there are more detailed explanations for each of the other 15± recommendations I made for RFKjr re the FDA and its EUA and Approval processes. Also just like here, the other recommendations make good medical and scientific sense.
Here is other information from this scientist that you might find interesting:
I am now offering incentives for you to sign up new subscribers!
I also consider reader submissions on Critical Thinking on my topics of interest.
Check out the Archives of this Critical Thinking substack.
WiseEnergy.org: discusses the Science (or lack thereof) behind our energy options.
C19Science.info: covers the lack of genuine Science behind our COVID-19 policies.
Election-Integrity.info: multiple major reports on the election integrity issue.
Media Balance Newsletter: a free, twice-a-month newsletter that covers what the mainstream media does not do, on issues from COVID to climate, elections to education, renewables to religion, etc. Here are the Newsletter’s 2024 Archives. Please send me an email to get your free copy. When emailing me, please make sure to include your full name and the state where you live. (Of course, you can cancel the Media Balance Newsletter at any time - but why would you?
Thanks for reading Critically Thinking About Select Societal Issues! Please pass a link to this article on to other associates who might benefit. They can subscribe for FREE to receive new posts (typically about once a week).
Thank you for making this issue a priority, John. I believe the FDA’s intentional use of RRR vs ARR for the vaccines (and in particular for Pfizer’s) is one of the most underrated deceptions of the entire Covid era. That “95% effective” claim was bandied about by everyone in media, the medical establishment, politicians and eventually by my own neighbors, friends and family. It was marketing genius, despite being completely misleading. In my early attempts to tell people about Relative vs Absolute risk, I wasn’t able to articulate it in a clear manner. No one understood, nor believed what I was claiming. Then the Canadian Care Alliance Pfizer presentation came out, which included a section on relative vs absolute risk (which you included at the end of your article - thank you!) and I began sharing that. It is the best explanation of Relative vs Absolute Risk hands down. Unfortunately, of the many people I’ve shared the video with, not a single one appeared to be moved or enlightened by the information (and this included my own doctor at the time!). Even more reason why things must change from the top down - the masses are too easily fooled and resistant to valuable information.
Thank you. Best explanation with charts I've seen. When I had tried the past 4 years to explain the difference to friends, their eyes glazed over immediately. But the difference of absolute vs relative vs NNT is HUGE and hugely important to grasp. Thank you